I am very excited to wish you a Happy New Year and to introduce myself to the C2C community of friends and supporters.
My name is Dr. Samuel Bernard and I recently joined the C2C team last month as the Chief Operating Officer. I completed my medical degree at the Faculté de Médecine et de Pharmacie at the State University of Haiti in 2009 and have completed additional health management studies at Montreal University. Most recently, I served as the Medical Director of the St. Boniface Foundation in southern Haiti.
I am thrilled to join the C2C team in Cap Haitien at this exciting time of growth and expansion. In 2018, we will open 3 new clinics in partnership with the Haitian Ministry of Health, doubling the size of the C2C network in the northern region. Both personally and professionally, I am a believer in C2C’s bold approach: providing the highest quality medical care at affordable prices.
In my country, we need to address urgent health financing challenges. Free care for every citizen, forever, just isn’t feasible and isn’t building the long-term economy. C2C’s is a different approach, we know that. But isn’t it exciting to think: What if a community clinic were a financially sustainable endeavor, delivering medical care today and in perpetuity? What if it didn’t have to rely on aid funding year after year? What if we built a solid economic foundation for the healthcare system in Haiti, rather than patching the holes?
As a physician, originally from Cap Haitien, I am passionate about returning to my home region to make a contribution to improving the health and wellness of people in northern Haiti. Over the past month, I’ve been rolling up my sleeves to get to know the communities we serve, family by family.
I am energized about what this year holds for C2C and invite you to join me in anticipating the achievements you will see us reach as the year unfolds!
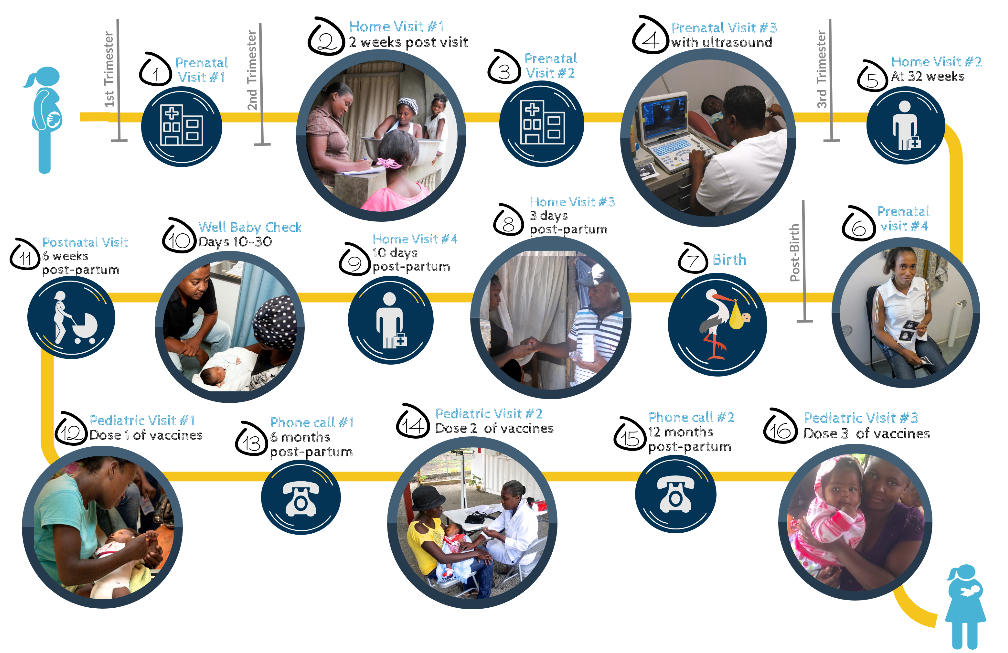
This holiday season, we are launching a new campaign to support the life-saving medical care we deliver to pregnant women and their babies in Haiti. It was our founding vision and motivation to ensure that poor women have access to the health services they need to have healthy pregnancies and thriving babies.
The Gift a Life campaign will support over 1,200 women through the journey of safe pregnancy and provide them with: a complete protocol of prenatal care, home-based and group-based education, robust postpartum care, and newborn care (including vaccinations) through baby’s first year.
How can you help?
You can donate to this campaign directly to give mothers and babies a healthy start in life.
Share this campaign with a friend, family member or colleague, and introduce them to this life-saving program.
Your support will make a real, lasting impact in the lives of so many vulnerable families. We look forward to sharing stories of health and success of the program as mothers and babies thrive in 2018.
Earlier this month, our Community Health Agents from the Acul du Nord and Camp Coq C2C clinics visited neighboring schools and pre-schools to distribute single-dose Vitamin A and Albendazole supplementation for children under 5 years old.
With the help of our partner Vitamin Angels, more than 350 children received immunization in the span of two days. Vitamin A can considerably reduce children’s risks of death from infection and diarrhea, and well as it aids in protecting their eyesight. On the other hand, Albendazole helps to boost children’s immune system by combating intestinal worms (de-worming).
Much of Haiti’s population, especially the most vulnerable– children, are infected with intestinal worms. These worms may consume some of their daily nutritional intake, causing malnutrition. In most cases, Haitians are infected by worms due to exposure to raw sewage, lack of clean water and access to health care. For many children, de-worming is the difference between life and death.
[slideshow_deploy id=’4571′]
C2C staff distributing vitamins to children in schools
Here at C2C, we love to highlight the amazing team members through a fun and informative Q&A. Get to know the newest addition to our staff, Ms. Alide Florvil!
Name: Alide Florvil
Where did you grow up? I was born in the Central Plateau, in a town called Hinche but when I was six years old I moved to Port au Prince with my sister until I was six years old. Then, I moved back to Hinch and lived there for most of my life. I grew up with both my parents but my oldest sister was also like a mother to me.
Where did you go to school? I did primary school in Port au Prince and then high school in Hinche. After high school, I went to auxiliary nurse school at the Edouard C. Joseph school in Hinche for 2 years. After graduating as an auxiliary nurse, I worked for a year at the Ste-Thérèse Hospital in Hinche but quickly found a job at World Vision where I was doing prenatal and postnatal consultations, training health agents and traditional birth attendants, and also visiting very rural and remote communities to bring health care. I worked at world vision for 7 years. After that, I decided to attend midwifery school as part of Midwives for Haiti’s one-year program. After graduation, I spent two years in the maternity ward at the Ste-Thérèse Hospital in Hinche and one year at MamaBaby Haiti before coming to C2C in July 2017.
What is your current title at C2C: NurseMidwife
What do you do at C2C? I do prenatal visits in the clinic and I am responsible for 4 maternal health agents- I trained them and supervise them as they conduct routine home visits with our pregnant patients participating in C2C’s expanded maternal health program. I am also responsible for enrolling women into the program and managing their care. I love my new job at C2C because I have many roles and responsibilities. It gives me the opportunity to learn new skills and share my knowledge with others.
How would you describe yourself? I am someone that is very open to others, I am not shy. I love asking questions and learn new things. I’m always open to criticism because that is how I learn. I love working in a team with others because you can share knowledge but also learn a lot from other people’s experiences and point of view. In general, I am someone that loves helping others and giving time to help those in need that don’t have the same opportunities as I have. My work doesn’t stress me out- I am always looking for new ways to have fun!
What do you do for fun or relaxation? I love to go to the beach and I also really love to dance. I wish I could go dancing more often. I also like to attend church every week.
Tell Us About Your Family (siblings/spouse/kids, etc): My parents are farmers, they had ten kids, I am the youngest. Now, I am married and I have 3 kids of my own. One girl, 16 years old, and two boys, 12 and 4 years old.
What job would you dislike or be really bad at? In life, there is no job that I would not do. I could do any job if I take the time to learn it. I enjoy learning new things. At the same time, there is no job that I would refuse to do, especially if I had to do a job to take care of my family. I believe that you should not refuse an opportunity that presents itself if it’s good for you and your family.
Why did you become a nurse midwife? Originally, my big dream was to become a doctor but my parents were farmers and were very poor. They had 9 kids before me, so they could not afford to pay for me to go to medical school. Eventually, I decided to go to auxiliary nursing school because it was the cheapest option but was still in the field of medicine. When I was younger, my father was always sick. He had stomach-related problems for a long time and I always took care of him, but I wished I could do more for him. That’s when I first got interested in medicine. After working as an auxiliary nurse for a long time, I came to realize that I was often faced with situations in the field where I could not help people because I did not have all the skills. Especially with pregnant women or women in labor. I decided to go to midwifery school so I can help more women and possibly save lives.
Who has influenced you the most in your career and why? The person that influenced me the most is my father. It is because of him that I decided to study and work in health care.
Meet the Staff is a new Q&A series that highlights the work, experience, and lives of staff at C2C.
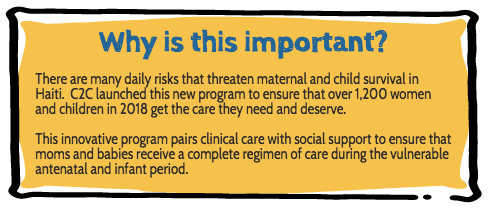
At C2C, we believe in “patient-centered care.” That means that we design our healthcare services according to the unique needs, preferences, and values of the patient population that we serve. Because our patients are poor and low-income people, we redouble our efforts to make sure that their voices are included in how we operate the clinics and how we define quality.
Recently, we asked our patients to give us feedback on their experience at C2C clinics. An independent evaluator administered surveys to hundreds of patients in August and we are proud to share the results with you!
Last month, C2C Co-founder, Elizabeth Sheehan, accompanied some of our Board Directors on a trip to visit our clinics in Haiti. The mission of the trip is to interact with C2C’s medical staff and engage in dialogue about perception and communication, patient interaction, and core values. The board team also toured C2C clinics in Camp Coq and Acul Du Nord, as well as the newest clinic in Cap-Haitien.
As an organization, C2C regularly measure and evaluate clinic performance to ensure we achieve our primary goal: to provide the best possible services to patients. The board along with C2C’s Haiti medical team participated in a series of workshops led by Dr. Calvaire, C2C Country Director, and Marie Marthe St. Cyr, C2C Board Director. Dr. Calvaire has extensive experience in medical practice and management. Ms. St. Cyr’s speaks fluent Haitian Kreyol and has a long history of promoting the social and economic empowerment of the Haitian community.
The workshops focused on the role of language and culture and how to effectively communicate with vulnerable people during patient interactions. Dialogue also explored the standard protocol for patient visits to understand how the care-provider can effectively apply C2C core values while educating and treating patients. These interactions give our teams the opportunity to make more effective clinical decisions while building strong long-term relationships with our patients.
Thanks to our partnership with Direct Relief, we received a shipment of medical supplies to ensure that our clinics are well-stocked with essential medicine to improve the lives of the most vulnerable families in Northern Haiti.
Direct Relief works to expand the availability of health services for all people through reliable and high-quality access to medicine, particularly to those who are most in need. Their commitment to C2C’s work strengthens our supply chain, which ensures that our clinics are never stocked out of medicine or supplies that our patients need.
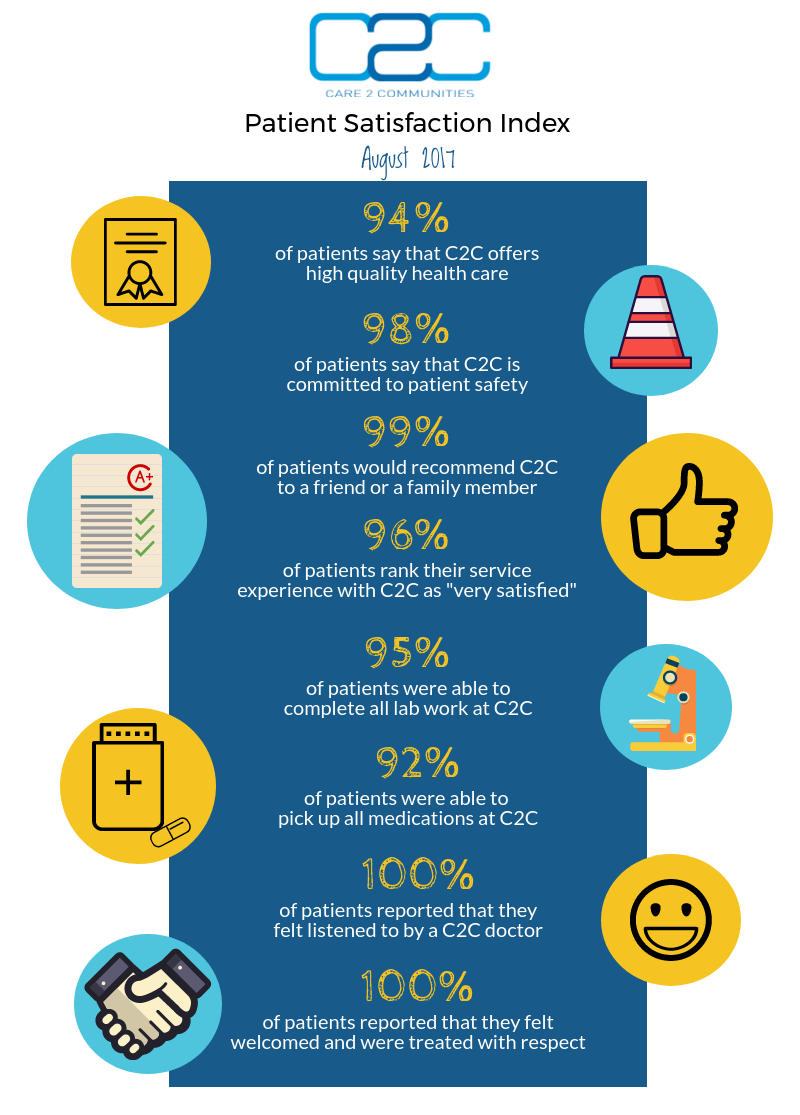
It gives us great pleasure to introduce our 2016 Annual Report, which sets out our achievements over the last year and our future plans.
With your support, we reached over 8,620 patient visits in 2016 and we expanded our programs to offer new, specialized services for pregnant women and malnourished children.
We’re proud of our impact in 2016, but mostly we feel deeply motivated to double our impact in the year ahead! We will open the doors of a new urban clinic in a few short weeks and planning is underway for a fourth clinic site in late summer. By the end of this year, the C2C network of community clinics will serve over 20,000 patients each year.
Please read more about our exciting expansion below!
According to the WHO, noncommunicable diseases (NCD), primarily cardiovascular diseases, cancers, chronic respiratory diseases and diabetes, are responsible for 63% of all deaths worldwide. 80% of NCD deaths occur in low- and middle-income countries. While the mortality rate remains high, NCDs are preventable through effective interventions that tackle shared risk factors.
Peter Piot, Director of the London School of Hygiene & Tropical Medicine and Trustee of the Novartis Foundation, recently wrote:
“Health systems in [developing countries] are ill-equipped to address this emergency. They are stretched under the pressure of fighting infectious diseases like malaria and tuberculosis, which still make up a majority of deaths in much of the developing world. It will take decades before sufficient health coverage is achieved that can adequately address the scale of the NCD epidemic. We need a new approach hks1njv.
We can draw some useful lessons from how HIV/AIDS patients were empowered to manage their condition. AIDS was the first experience of managing a ‘chronic’ condition that many low-and middle-income countries had. With the introduction of antiretroviral therapy from the mid-1990s the life expectancy of many AIDS patients increased. Many were able to return to their lives and families instead of being hospital-bound.
Faced with the prospect of having to care for these patients for potentially a very long time, public health systems mobilised to empower AIDS patients to self-manage their condition with appropriate support from their physicians. This shift to a patient-centered approach – taking chronic care outside of the formal healthcare system and hospitals, and into the community and families – has eased the burden of tackling the epidemic and led to precious resources reaching more people.”
This is where innovation in healthcare can contribute to solving the NCD problem. C2C has developed a health care delivery system that is built around patients. Our patient-centered care model is often the point-of-entry to the care system for vulnerable people and families. We respond to local health needs by drawing on communication between the community and the clinic. At C2C, we believe that this approach is fundamental to effective primary care as we help Haitian families get well and stay healthy.
Entrepreneurs love the concept of disruption in the market. Silicon Valley defines “disruption” as a simpler, cheaper or more convenient alternative to an existing system or product. When it comes to delivering quality healthcare in the developing world, disruption simply isn’t the answer.
Dr. Caroline Buckee said it best in her Boston GlobeOp-ed: “When it comes to addressing epidemics — and a lot of other global challenges — the Silicon Valley startup mentality doesn’t work.” Disruption has become a trend in many spaces among innovators. As for the global health care space, we see more grant guidelines calling for this sort of mentality and problem-solving. While it’s important to encourage innovation in healthcare, we should keep in mind that health care delivery, when supported, is an effective solution to saving lives. As Dr. Margaret Chan, World Health Organization Director-General once said, “a primary health care approach is the most effective way to organize a health system.” At Care 2 Communities, we believe that primary care works. When patients have access to high-quality, affordable, reliable healthcare, it means that mothers are able to care for their children, children can stay in school, and the entire community benefits economically from a healthy workforce.